Medicaid work requirements leave states scrambling for 2027
By Michael McAuliff / March 10, 2026
President Donald Trump and the Republican led-Congress cut nearly $1 trillion from Medicaid last year. Now it’s up to the states to carry out work requirements and other complex policies.
The work requirements, new eligibility standards and processes, and other rules stemming from Trump’s tax law begin to kick in Jan. 1, 2027. For policies this consequential, that’s a blink of an eye, and states are scrambling to create regimes that will affect providers around the nation with varying levels of intensity.
In addition to the mandates on states, the law restricts their ability to levy taxes on providers to finance Medicaid and their ability to impose state-directed payments that set minimum provider reimbursements for Medicaid managed care contractors.
“They’ve been handed an almost impossible task here to get this policy up and running by Jan. 1,” said Joan Alker, executive director of the Georgetown University Center for Children and Families. “Even if their state doesn’t want to do it, they’re now mandated to do it.”
All 50 states, the District of Columbia and U.S. territories must prepare for the law, and their responses are differing widely. The 10 states that didn’t expand Medicaid eligibility to working-age adults under the Affordable Care Act of 2010 face the lightest challenges because the tax law enacts more requirements and restrictions on expansion states.
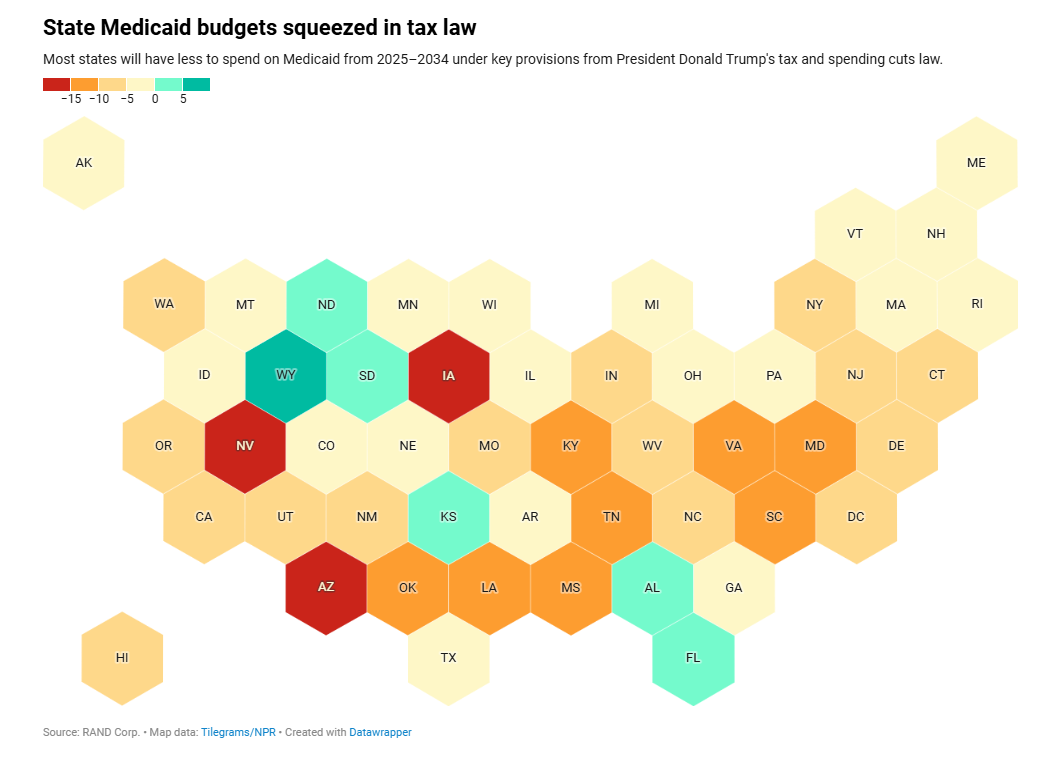
The tax law is projected to reduce federal Medicaid funding by $960 billion over 10 years. The fiscal consequences for states are significant and varied. Twenty states will see their federal Medicaid support diminish by at least 5%, according to an analysis from the Rand Corp. That is likely to translate into cuts on providers and beneficiaries.
The new, stricter eligibility and enrollment processes and the work requirements need to be in place by next year. Most states’ fiscal years begin July 1, meaning they must act quickly to enact the laws and regulations necessary to be ready.
That task is complicated by the fact that the Centers for Medicare and Medicaid Services has not issued detailed guidance advising states on how to implement the tax law provisions. The agency’s official, binding guidance is not due until June.
“It’s really going to be incumbent on the administration, for this to succeed, to be kind of trickling out a whole lot of sub-regulatory guidance and other types of hints and winks and nods along the way, because the clock is ticking,” said Matt Salo, CEO of Salo Health Strategies and former executive director of the National Association of Medicaid Directors.
States have myriad choices to make and innumerable technical and policy considerations to work out. They must procure and activate the technological systems required to comply with the law’s enrollment and work requirement processes, decide how strictly to enforce the work requirements, and devise plans to inform providers and enrollees of the new rules.
“You’ve got to do a lot of things, ranging from making big picture political decisions of exactly how are you going to roll this thing out, to how aggressive do you want to be?” Salo said.
In the meantime, states, providers and anyone else with a stake in these policies should stay aware of the evolving politics, Alker said.
“This is a very high-profile political issue, we’ve got elections coming up, and so the White House is going to have the final say on what’s in the rule,” Alker said.
Arkansas attempted a work requirements program in 2018 that saw 18,000 people lose coverage before federal courts shut it down. The state is deep in the weeds on the latest iteration, said state Department of Human Services Secretary Janet Mann.
“We are working on system changes. We are working on a communication tool kit. We are working through a lot of the policy decisions that we are making right now,” Mann said.
Arkansas is making rapid progress setting up the systems to validate if Medicaid enrollees are abiding by the requirement that they work at least 80 hours a month, Mann said.
The previous experience taught Arkansas that undertaking robust communications through every means available is critical, Mann said.
While states await more detailed federal guidance, they can keep close eyes on what their counterparts are doing and maintain contact with stakeholders. In Arkansas, the state is conducting outreach to interested parties, such as the Arkansas Hospital Association, Mann said.
Conceptually and politically, state leaders have an overriding choice to make: Whether to err on the side of keeping eligible people enrolled or err on the side of blocking ineligible people from getting Medicaid, Salo said.
States such as Pennsylvania had already been reaching out to stakeholders in hopes the state would choose the first path, while policymakers in places such as Nebraska and Idaho appear to be leaning the other way, said Katherine Hempstead, a senior policy advisor at the Robert Wood Johnson Foundation, a philanthropy that finances health research.
“They are two states that want to even kick it up a notch and do everything that the feds want them to do and more,” Hempstead said.
Nebraska is gunning to have its work requirements system running by May 1, eight months early. Idaho Gov. Brad Little (R) has already proposed cutting $22 million in Medicaid spending to prepare for the law, likely impacting home- and community-based services for people with disabilities.
“That’s a part of the Medicaid budget that is vulnerable when there are kind of general cuts,” said Hempstead. “Services for people with disabilities and low-income, elderly people, people with intellectual disabilities — they have services in Medicaid that are really important and are pretty expensive."
Providers should monitor what happens in Nebraska and steel themselves for cuts like those under consideration in Idaho as states endeavor to balance their budgets, Hempstead said. Georgia, which has a form of work requirements in place, may also offer lessons.
Physicians and others also may be called upon to participate in the work requirements system.
“They will have some responsibility on helping members make sure that they’re still enrolled or that they’ve gotten the data that they need to be verified,” Mann said.
States will have to determine how to implement the tax law’s exemption from work requirements for people deemed “medically frail,” a term the statute does not define. Since this status must be validated, providers will be involved.
Arkansas can use current beneficiaries’ claims history, but new enrollees present a challenge, Mann said. “How do we obtain that data to make a medical frailty determination? In some cases, I think it’s just nuanced,” she said.