The Art and Science of Medicaid Budget Forecasting
By Neda Jasemi / April 28,2026
Forecasting state and territory Medicaid budgets will be especially difficult this year, as changes in healthcare utilization, underlying costs, new treatments, and eligibility policy are reshaping the parameters of the program and introducing greater uncertainty into the forecast. Six years after the start of the COVID-19 pandemic and three years after the nationwide unwinding began, Medicaid agencies are still working to understand the program’s “new normal” as they forecast enrollment, utilization, and administrative costs that shape the Medicaid budget. In addition, expansion states are implementing significant eligibility policy changes (e.g., work and community engagement requirements, six-month redeterminations) that will impact federal revenue, enrollment, and per-member costs for future fiscal years.
To peel back the curtain on the complex process of Medicaid forecasting, the National Association of Medicaid Directors (NAMD) conducted interviews with several state Medicaid financial leaders exploring four aspects of forecasting:
Why Medicaid Forecasting is Important, including Medicaid’s outsized impact on the state budget and the consequences of even a small forecast deviation in such a large budget category.
The Process to Forecast Expenditures, including reliance on quality data and mature data streams that allow Medicaid agencies to conduct front-end budget development, track expenditures, and refine methodology.
The Top Challenges in Forecasting, which typically result from a lack of high-quality historical data that can be used to predict future enrollment, utilization, and overall spending. This can occur when the Medicaid agency is navigating new policy, public health events, or operational challenges to aggregate data timely and effectively.
State Innovations, including consensus forecasting, comprehensive cost reporting, and strategies to improve statistical methodology, IT expenditure projections, and the quality of encounter data.
Notably, Medicaid forecasting can never be entirely certain because the program is constantly evolving. In addition to refining their methodologies and improving data quality, Medicaid agencies also implement policies and processes designed to mitigate fiscal risk associated with this uncertainty.
States organize their Medicaid finance shops in different ways. In some states the Medicaid agency is responsible for all aspects of forecasting, including data aggregation, analysis, and budgeting, along with expertise in Medicaid policy and financing. In other states some of these responsibilities are split between the Medicaid agency and the larger state health and human services department (e.g., Medicaid agency is responsible for data aggregation and analysis, while the larger department is responsible for budgeting). All of these factors influence processes, challenges, and innovations in budget forecasting so insights from this brief may have varying applicability across states.
Why Medicaid Forecasting is Important
Because Medicaid makes up a large portion of the state budget, even slight deviations between the Medicaid forecast and actual spending can impact the state budget.
Accurate forecasting is therefore critical not only for Medicaid program management, but also for many other programs states fund. States generally must balance their budgets over one- or two-year budget cycles, meaning that they cannot spend more during the budget cycle than they collect in revenue. Illustrating this point, one Medicaid financial leader quoted an old saying from a former governor: “If Medicaid sneezes, the whole state gets the flu.”
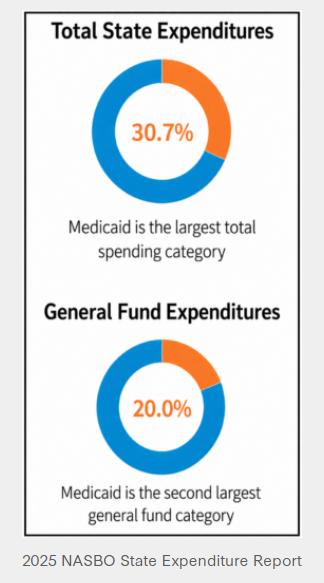
According to the National Association of State Budget Officers, in fiscal year (FY) 2025:
Medicaid made up 30.7 percent of total state expenditures across states, which is the largest spending category in the state budget. Total state expenditures reflect all spending, including from federal, state, and local-generated revenues.
Medicaid made up 20.0 percent of general fund expenditures across states, which is the second largest general fund category after education. General fund expenditures reflect spending from state-generated revenue.
How States Forecast Medicaid Expenditures
While each state’s forecasting process differs slightly, forecasting generally includes three phases: 1) front-end budget development; 2) tracking expenditures on a regular cadence; and 3) retesting and refining methodology. Medicaid agencies typically forecast expenditures, not revenue, unless it’s through Medicaid-specific financing mechanisms like provider taxes. Typically, there are other agencies in state government (e.g., department of revenue) that forecast revenue for the state.
1. Front-End Budget Development
Before the fiscal year begins, Medicaid agencies develop and submit an agency budget to their governor’s office and then to the legislature for approval through the appropriations process for the coming year. As a result, Medicaid agencies typically forecast expenditures more than a year before the fiscal year starts. Because states generally operate either under an annual or a biannual budget, front-end budget development could have a one-to-two-year outlook.
The forecast includes projections for enrollment (i.e., Medicaid members enrolled per month), utilization (i.e., amount of healthcare costs per member per month), and administrative expenses (i.e., operational and system costs to administer the program). Of these factors, enrollment and utilization have the greatest impact on forecasted expenditures.
Medicaid forecasting relies heavily on high-quality historical data, including claims and encounter data, eligibility data, and, in some cases, information from a state’s accounting system. Because data flows and quality differ between managed care and fee-for-service delivery systems, states often use different processes to forecast utilization across these delivery systems. For instance, states collect managed care data through encounters, which can lag or have varying levels of completeness and data quality depending on the state, the managed care organization (MCO), and type of service delivered. States account
for these limitations through targeted data requests and analyses from MCOs, as well as actuarial methods such as incurred but not reported (IBNR) claims and other techniques to estimate missing or incomplete real-time data. Meanwhile, fee-for-service claims data are also subject to lag, as providers may submit claims long after services are delivered or in batches. Ultimately, states depend on robust Medicaid Management Information Systems (MMIS) and data warehouses to support these analyses.
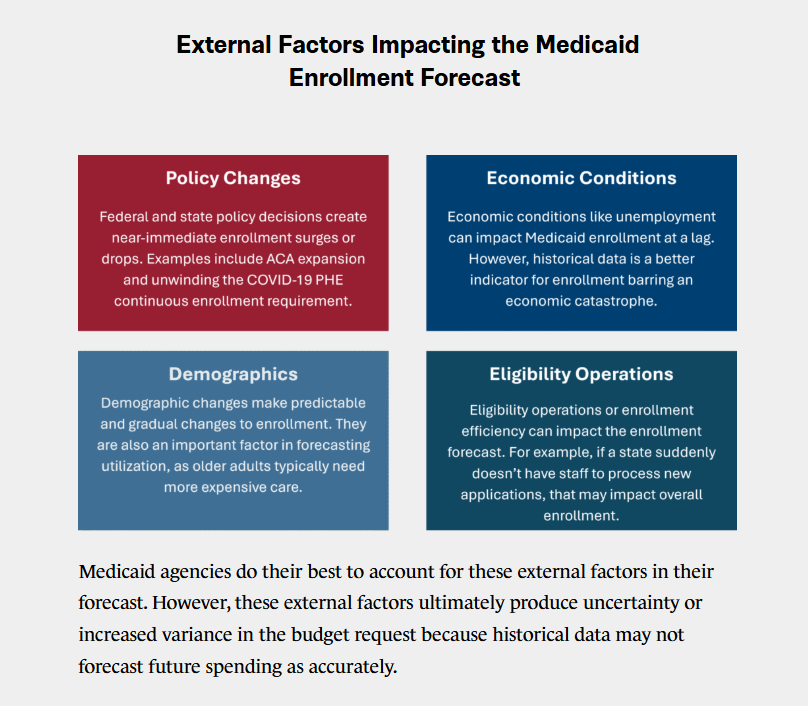
A state’s historical expenditures, enrollment, and utilization trends are often the strongest indicators of future spending. Using this data, Medicaid agencies use statistical methodologies to project expenditures for the upcoming fiscal year. However, Medicaid agencies must also account for external factors when developing their final forecasts. This requires deep knowledge of the program’s policies, operations, and emerging trends. In some cases, leadership may adjust model inputs to ensure projections reflect expected program changes and produce outputs that are realistic given what they know about the Medicaid program.
One Medicaid financial leader highlighted four factors that impact the enrollment forecast including policy changes, economic conditions, demographics, and eligibility operations.
2. Tracking Expenditures on a Regular Cadence
After the legislature appropriates funds, Medicaid agencies track spending, utilization, and enrollment throughout the fiscal year to assess the accuracy of their projections and monitor expenditures relative to general funds and state revenue cycles. Medicaid agencies track spending and utilization weekly or monthly (processes and cadence typically differ between managed care and fee-for-service).
The purpose of tracking expenditures against the forecast is to reduce fiscal risk by quickly identifying whether the program is overspending or underspending compared to their initial projections. Given the proportion of state budgets devoted to the Medicaid program, knowing exactly how much the program is spending and when it is spending it is critical from a budgetary perspective.
If the Medicaid agency is overspending compared to the initial forecast, they can take quick action to make policy changes, mid-year adjustments, or implement other strategies to control costs. If necessary, the Medicaid agency may have to work with other state policymakers to pass a supplemental budget, reallocate funds, or adjust appropriations. These actions reduce risk to the overall budget and maintain the balanced annual or biannual budget.
3. Refining Methodology
Some states will reexamine their model during the budget cycle to improve next year’s forecast. States sometimes test their models against actual spending to refine their forecasting methodology. While this process can overlap with the following year’s budget development, methodological improvements can improve the long-term accuracy of budget forecasting.
Top Challenges in Medicaid Forecasting
Challenges in Medicaid forecasting generally stem from a lack of quality historical data. Broadly, these challenges fall into three categories including 1) new policy, 2) unprecedented public health events, and 3) aggregating data timely and effectively.
1. New Policy
New policy that shifts enrollment, utilization, and payment rates can introduce additional complexity into Medicaid budget forecasts. Because historical data cannot capture the effects of new policy developments, these shifts introduce significant uncertainty into the forecasting process.
For example, when states stood up adult expansion, they had to rely on less robust data sources as opposed to more thorough internal Medicaid data for the new population. As a result, they made high level estimates based on their current program, current population, and survey data. They also had to estimate what percentage of the eligible population would apply for the program. Because these estimates weren’t based off historical data within the program (e.g., claims and encounter data), they introduced more uncertainty into the forecasting process and some states underbudgeted for expansion. As states gained more experience and data about this population, they were able to forecast enrollment and utilization with more certainty.
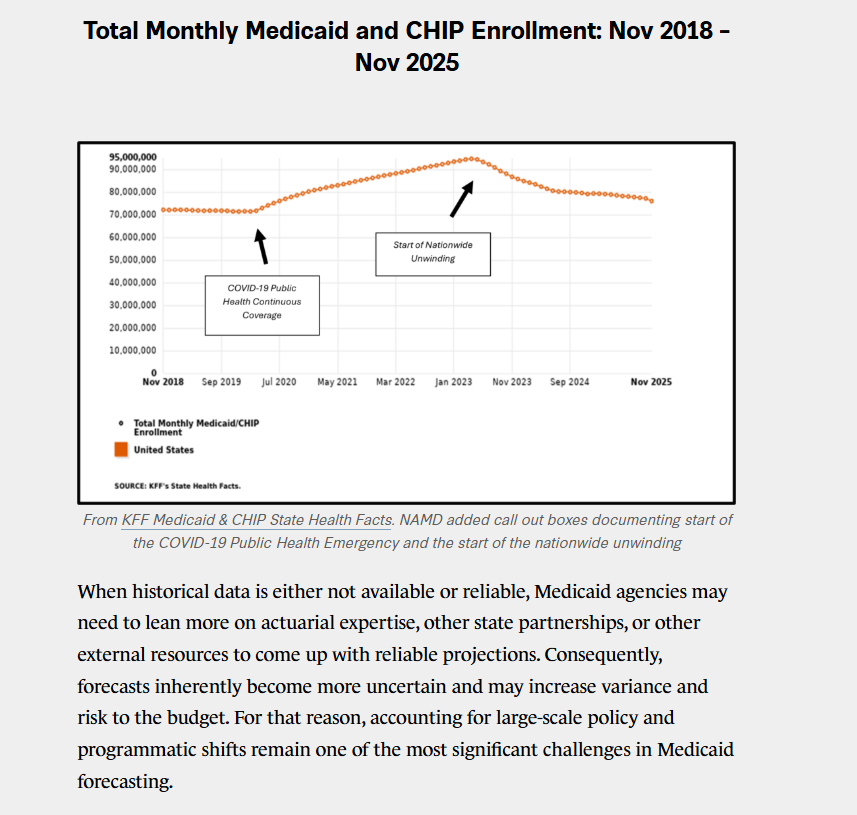
Similar enrollment forecasting challenges occurred during the unwinding of the federal continuous coverage requirement, where states redetermined eligibility for all enrolled members who retained coverage during the COVID-19 Public Health Emergency (PHE). Because states had no prior experience with this type of policy change, historical data could not reliably predict how many individuals would disenroll, how quickly they would disenroll, or what average per-member costs would look like. Now, two years after the end of the unwinding process, enrollment remains higher than pre-pandemic levels, and the population that remains enrolled in the program has higher healthcare needs (i.e., higher acuity), resulting in higher average per-member per-month costs. All experts interviewed for this brief emphasized that the nationwide unwinding introduced significant forecasting challenges due to its unprecedented effects on eligibility and utilization.
2. Unprecedented Public Health Events
Unprecedented public health events can change how members utilize healthcare, which can create uncertainty in the Medicaid budget forecast. One notable example is the COVID-19 PHE. Hospital utilization rose during the peak of the pandemic, but Medicaid agencies are still evaluating the pandemic’s longer-term effects on how people use healthcare. One Medicaid financial leader highlighted three areas where there may be longer-term shifts in utilization:
Telehealth. While lower than its 2020/2021 peak, telehealth utilization remains well above levels from the late-2010s. The pandemic may have accelerated adoption of telehealth as current use reflects a sustained shift in healthcare delivery.
Behavioral Health. The pandemic may have exposed and intensified an underlying behavioral health crisis. Increased demand has not returned to pre-pandemic levels, and utilization continues to run high. Behavioral health remains one of the most dynamic areas of the healthcare landscape and a key trend to monitor.
Long-Term Care. The pandemic accelerated the shift from nursing facilities to home and community-based services (HCBS). That shift will likely have lasting implications for long-term care delivery. As the baby boomer generation ages, uncertainty remains about how durable the move toward HCBS will be and implications for future demand and spending.
Medicaid agencies are still assessing the “new normal” for healthcare utilization after the COVID-19 PHE. The volume and type of healthcare people consume has changed, so Medicaid agencies have to respond to new and evolving data in the forecasting process.
Finally, unrelated to the pandemic, the pipeline of new prescription drugs, such as cell and gene therapies and GLP-1s, is a growing focus of the forecasting process. Some key considerations include price points, the size of the Medicaid population eligible for these new treatments, anticipated utilization, and downstream effects on other Medicaid services and supports. As the pipeline of high-cost treatments grows, there may be more volatility in Medicaid budgets and budget forecasts.
3. Aggregating Data Timely & Effectively
Because the forecasting process is based on continual analysis of pricing, utilization, and operational data, Medicaid agencies can experience operational challenges aggregating data timely and effectively. This can occur when data is spread across multiple entities, such as different state agencies and county governments.
For example, many counties operate specialty behavioral health services that serve both Medicaid members and non-members. The Medicaid agency may not always have line of sight into entity-specific fee schedules, operations, and utilization. Therefore, the Medicaid agency may rely on annual survey data or less-mature data feeds with each entity to gather the relevant data needed to inform the forecast. This can be lengthy and complex, whereas forecasting is more seamless when a single entity centralizes the data, or when the Medicaid agency has mature data feeds.
Similar challenges can arise with eligibility data, impacting enrollment projections. For instance, some states rely on counties to operate eligibility and enrollment operations. While the Medicaid agency is responsible for eligibility policy, they would need to collect and aggregate data to have full line of sight into daily operations, staffing levels, and processes for each county. These factors are important to forecasting enrollment because they impact how quickly people enroll in the program.
Because Medicaid forecasting relies on high-quality and up-to-date data, operational issues in collecting information that impacts utilization and enrollment can pose a challenge when forecasting expenditures. Medicaid agencies are working with their counterparts to improve data flows and information sharing to strengthen the forecasting process.
Examples of State Innovations
To better understand how states are improving their forecasting, we asked state experts interviewed for this brief to highlight examples of program innovations. The examples below present a non-exhaustive list of forecast improvement activities.
Improving Statistical Methodology
States continue to strengthen their statistical methodologies to improve forecast accuracy. For example, this can include testing the forecasting model each year and using historical datasets to assess how accurately the model predicted prior expenditures. Based on these results, the team refines the model to improve future forecasts.
One Medicaid financial leader highlighted the use of new statistical tools and machine learning approaches that place greater weight on more recent data than older experience. For example, using TBATS (Trigonometric terms, Box-Cox transformations, ARMA errors, Trend, and Seasonal) models to better capture nuances in healthcare utilization and enrollment trends. Moving forward, some states are exploring how artificial intelligence (AI) and predictive analytics can strengthen their forecasts, such as using AI-assisted tools to assign probabilities to forecast scenarios that would inform recommendations to key policymakers.
Consensus Forecasting
Many states use consensus forecasting, which brings together fiscal experts from the legislative branch, the state budget office, and the Medicaid agency to estimate Medicaid expenditures. Consensus forecasting requires collaboration between the executive and legislative branches to create better accountability and transparency across branches of government. While each state has unique experiences and unique politics, one Medicaid financial leader highlighted that, in their state, consensus forecasting helps keep forecasting discussions focused on analytical methods rather than political considerations.
Predicting IT Expenditures
States continue to improve data visibility and better track IT system expenditures. For instance, the Medicaid budget director in Tennessee joins key meetings when the IT team is developing, iterating, or making changes to their systems. As finance staff become more conversant in IT systems work, they are able to more accurately forecast these administrative costs. The fiscal team is also able to quickly identify when IT system projects are going awry, and when they need to adjust the budget. Collaboration between IT and finance also helped the state use their financial levers to promote accountability and predictability with vendors. For example, Tennessee pays IT vendors through a milestone reimbursement approach, where vendors are paid a certain amount for a given milestone, regardless of how long it takes the vendor to achieve that milestone.
Comprehensive Cost Reporting
Many states conduct comprehensive cost reporting and splice data to observe cost trends within specific populations. Sophisticated reporting can examine all Medicaid costs by service category on a per-member per-month basis, which allows the Medicaid agency to quickly pull spending data on a specific service and break it down by eligibility group. This capability allows the Medicaid agency to conduct ad-hoc analyses and quickly forecast impacts of various policy proposals.
Encounter Data Quality Initiatives
Medicaid agencies continually improve data quality with MCOs, which is a key component of capitation rate development and thus forecasting. For example, on a quarterly basis, Michigan compiles the encounter data submitted by MCOs and shares it back with them, showing how the state interprets and uses the data. MCOs are then asked to compare the state’s interpretation with their own records to identify any discrepancies. This process creates a continuous feedback loop that improves the quality and consistency of encounter data submitted to the state. Improving this data quality supports both Michigan’s rate-setting and rate-adjustment processes. Prior to implementing this approach, resolving discrepancies often required significant back-and-forth between the state and MCOs. By identifying and addressing issues earlier in the process, Michigan resolves discrepancies more efficiently and keeps discussions focused on the data.
So What?
Medicaid forecasting is both a technical and strategic function within state and territory government. It requires quality data, rigorous analysis, and expertise in the policies, programs, economic conditions, and human behaviors that shape how people enroll in and use Medicaid healthcare services. As states navigate shifting utilization patterns and an evolving policy environment, forecasting will remain an essential tool for planning and decision-making. While uncertainty is part of budget forecasting, particularly in a period of significant change, Medicaid agencies bring together fiscal, policy, and program experts with deep knowledge of the program. Their expertise enables states to navigate uncertainty, manage fiscal risk, and ensure Medicaid can continue to help millions live their healthiest lives and make the most effective use of taxpayer dollars.