340B Reform, Medicaid Fraud, and Rising Costs
By Brian Blase / May 13, 2026
Reforming 340B
The 340B Drug Pricing Program—originally intended to support safety-net hospitals serving low-income patients—has evolved into one of the most distortionary and least transparent programs in health care. In a new prognosis, Jackson Hammond explains how 340B has fueled hospital consolidation, increased health care costs, and rewarded large hospital systems at the expense of patients and truly struggling providers.
Created in 1992, 340B requires pharmaceutical manufacturers to provide steep discounts on drugs to qualifying hospitals and health centers. Hospitals then administer those drugs and are reimbursed at much higher rates, allowing them to keep the difference. What began as a relatively small program has exploded in size. Discounted 340B drug purchases increased from $5 billion in 2010 to more than $81 billion in 2024, while the number of participating hospitals and contract pharmacies has surged.
The incentives embedded in the program have reshaped the health care market. Because hospitals profit more when they administer larger volumes of higher-cost drugs, the program has become a major driver of consolidation as 340B hospitals are incentivized to acquire physician practices and other competitors in order to increase drug volumes. Research shows 340B contributes to higher drug costs, higher insurance premiums, and increased hospital ownership of outpatient facilities and physician practices. Rather than strengthening care in underserved communities, hospitals often use 340B revenues to expand into wealthier, commercially insured markets.
Hospitals are generally not required to disclose how much money they generate through 340B or how those funds are used, even as many small rural and inner-city hospitals continue to struggle financially.
The Trump administration proposed a 340B rebate pilot that would have required covered entities to share claim‑level data with participating manufacturers to confirm that a drug was not also subject to a Medicare Maximum Fair Price discount or a separate 340B rebate on the same claim. Hospitals sued to block the pilot before its planned January 2026 start, and a court halted the pilot, finding that the administration did not provide sufficient opportunity for stakeholder input. The administration ultimately abandoned the pilot but later issued a request for information in February on whether and how to move forward with a revised version.
Jackson argues that policymakers should move beyond modest transparency reforms and fundamentally restructure the program by eliminating the “buy low, bill high” spread that drives consolidation and inflates costs. A reformed system should instead direct support based on a hospital’s actual provision of charity care and services to vulnerable patients.
A Conversation with the Congressional Budget Office
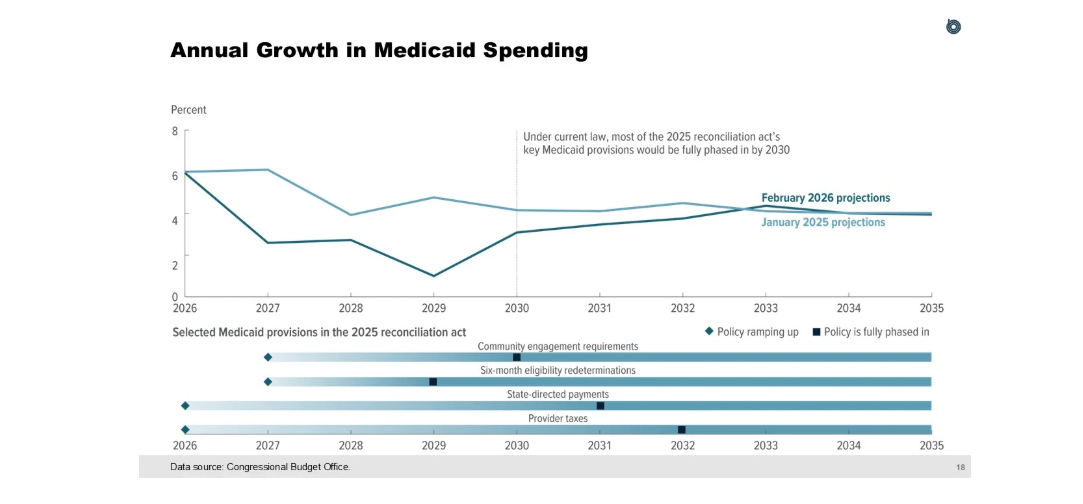
On Monday, Paragon hosted Phillip Swagel, the director of the Congressional Budget Office (CBO), and several members of his team for a discussion of CBO’s baseline projections of federal subsidies for health insurance. CBO’s presentation is here. I opened the discussion on the importance of putting federal health programs on sustainable footing and 2023 Paragon research that federal health programs need nearly $2 trillion of savings relative to baseline to put the federal budget back on a sustainable trajectory.The good news is that the One Big Beautiful Bill contains more than $1 trillion in projected health care savings. The bad news is that the underlying baseline was much higher in 2026 than expected in 2023. Much of the increase stems from Affordable Care Act exchange enrollment growth, with much of it improper; growing corporate welfare in Medicaid; and the Inflation Reduction Act (IRA) substantially increasing Medicare Part D spending. There were two particularly compelling figures from CBO’s presentation. First, according to CBO (and illustrated by this figure), the OBBB will not result in any annual reductions in federal Medicaid spending ever. Counter to the misleading narrative of “Medicaid cuts,” federal Medicaid spending will grow every year—just a bit more slowly from 2027-2032 because of the important reforms in the OBBB.
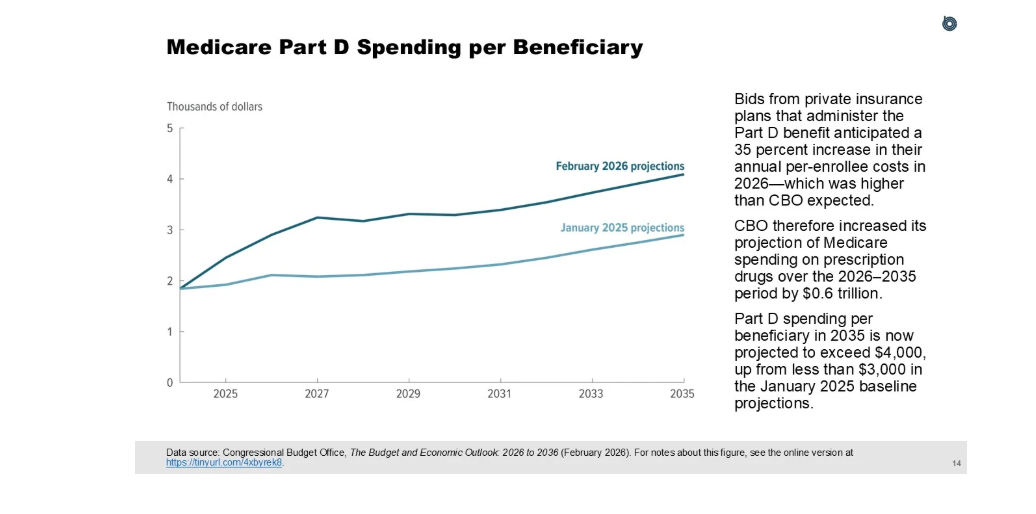
Second, the IRA has caused Medicare Part D expenditures to explode. According to CBO, the poorly developed Part D redesign is costing much more than expected and the drug negotiations are saving less than expected. CBO now expects Part D will cost taxpayers $669 billion more than it projected just last decade. CBO’s next figure shows that it expects Part D per-enrollee spending to be more than one-third higher than it projected last year.
Medicaid and Medicare Fraud Everywhere
In just the past few weeks, federal prosecutors and investigative journalists have surfaced a striking range of health care fraud schemes:
$46.6 million skin substitutes fraud scheme: On April 28, DOJ announced the seizure of more than $2 million from a California wound care clinic accused of billing Medicare for skin grafts and skin graft substitutes that were never actually performed on patients. The clinic billed more than $46.6 million for services purportedly provided to 78 beneficiaries—at rates more than double the national average per claim—and Medicare paid approximately $34 million on the claims.
$522 million genetic testing fraud scheme: On May 4, DOJ announced the sentencing of two men who ran labs that paid kickbacks to marketers to collect DNA samples from insured patients and to medical providers who signed fraudulent orders for medically unnecessary genetic tests—disguising the payments as marketing services through sham contracts. The laboratories billed about $522 million in fraudulent claims to Medicare, Medicaid, and private insurers, which paid roughly $84 million before the scheme was uncovered.
Daily Wire investigation exposed Medicaid home health fraud in Ohio: Using newly public Medicaid spending data released by DOGE in February, the investigation found that Ohio spent roughly $1 billion on home health care in 2024, with one nearly empty Columbus office complex alone housing 94 home health companies that collectively billed taxpayers about $66 million.
$197 million DME fraud scheme: On May 8, DOJ announced the sentencing of a former NFL player for a yearslong scheme to defraud Medicare and the VA’s CHAMPVA program out of nearly $200 million through fraudulent billing for orthotic braces. He used overseas call centers to pressure elderly patients into accepting unnecessary braces, paid kickbacks to sham telemedicine companies for signed doctors’ orders from providers who never examined the patients, and billed the programs through eight durable medical equipment (DME) companies while hiding his ownership from Medicare.
Fox News report flagged a Medicaid autism-therapy billing surge in North Carolina: According to Fox News, North Carolina State Auditor Dave Boliek warned of potential waste, fraud, and abuse in the state’s Medicaid program after autism-therapy billings jumped roughly 47,000 percent in five years—from about $1.4 million to more than $660 million annually—with state data showing Applied Behavior Analysis (ABA) therapy spending grew 347 percent between 2022 and 2025 and is projected to hit $1.14 billion by fiscal year 2027. The pattern echoes Minnesota’s autism therapy fraud scandal, where the state’s program grew from $3 million in 2018 to nearly $400 million in 2023 before federal agents started uncovering widespread fraud.
These cases are only the latest examples of systemic vulnerabilities in federal health programs. New fraud schemes surface almost every week. To follow the full picture of health care fraud, visit Paragon’s Health Care Fraud Dashboard.
Limited Excepted Benefit for Fertility Treatments
On May 10, the Department of Labor (DOL) proposed a new rule that would create a limited excepted benefit for fertility treatments and related services. Limited excepted benefits are those that are exempt from federal health insurance requirements, so long as those benefits are provided under a “separate policy, certificate, or contract of insurance, or are otherwise not an integral part of a plan.” The limited excepted category includes benefits excluded from the primary health plan or offered under a separate plan, such as vision or dental coverage.
The proposal is intended to reduce regulatory burdens and increase flexibility for employers that want to offer fertility benefits. The proposed rule would allow individuals who may be on a spouse’s health plan to enroll in fertility coverage through their own employer without enrolling in their employer’s main health plan. The benefit is capped at a lifetime limit of $120,000, which will be indexed to inflation starting in 2028. DOL’s regulatory impact analysis projects this policy will nearly double the number of employers offering fertility benefits.